
News | AP VALVES & SH 2023
14-Year’s Journey of AMC TAVR
“TAVR has become the standard of care for patients with symptomatic severe aortic stenosis, regardless of age or specific cases.”
Seung-Jung Park, MD, PhD (Asan Medical Center) presents the 14-year journey of TAVR in the opening session during the 12th AP VALVES & STRUCTURAL HEART 2023 held at the Grand Walkerhill Seoul, South Korea on August 10.
As of 2023, the 2020 ACC/AHA guideline recommends TAVR for severe symptomatic Aortic Stenosis (AS) patients over the age of 65, while those under 65 are considered for Surgical Aortic Valve Replacement (SAVR) based on their age. However, the 2021 ESC/EACTS guidelines recommend TAVR for patients over 75 years of age, with all other patients evaluated for either TAVR or SAVR based on their specific condition. Dr. Park now suggested that TAVR is the primary choice for patients in need of a tissue valve, with SAVR considered for those deemed unsuitable for the TAVR procedure.
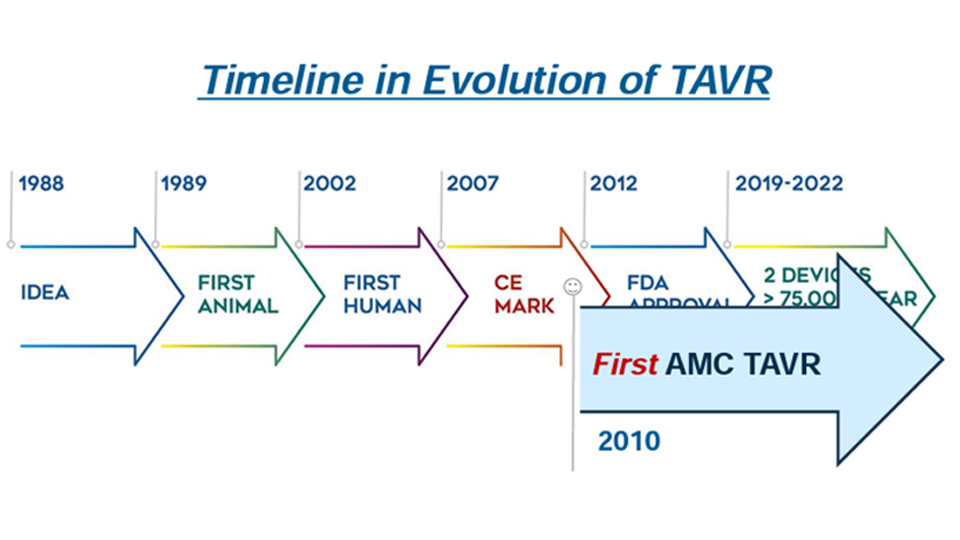
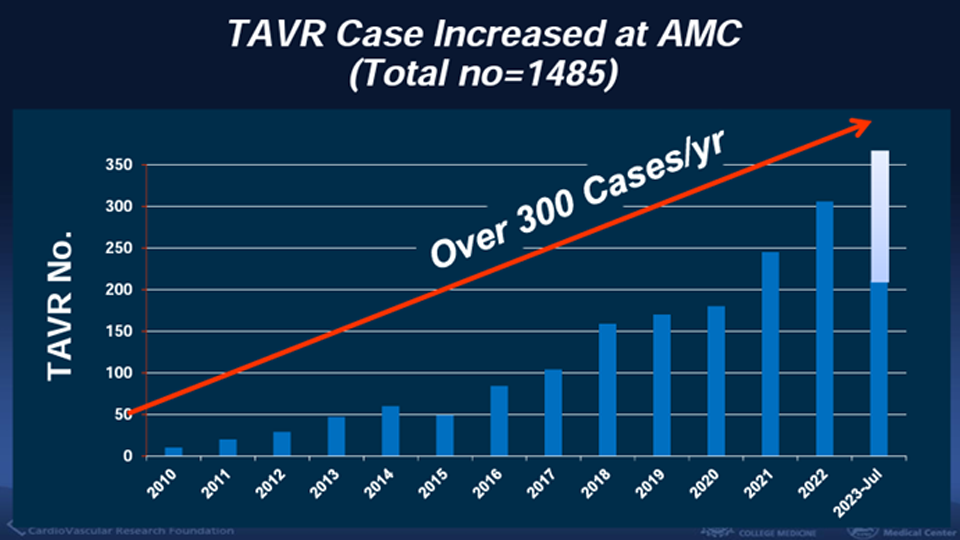
Asan Medical Center, which initiated TAVR procedures in 2010 and currently performs approximately 300 TAVR cases per year, totaling over 1500 cases, has achieved promising outcomes. These outcomes include procedural success rates of 99.5%, with low mortality (1.3%), stroke (0.3%), vascular complications (4.2%), permanent pacemaker insertion (6.8%), moderate to severe paravalvular regurgitation (0.4%), and more, showcasing the effectiveness of their approach.
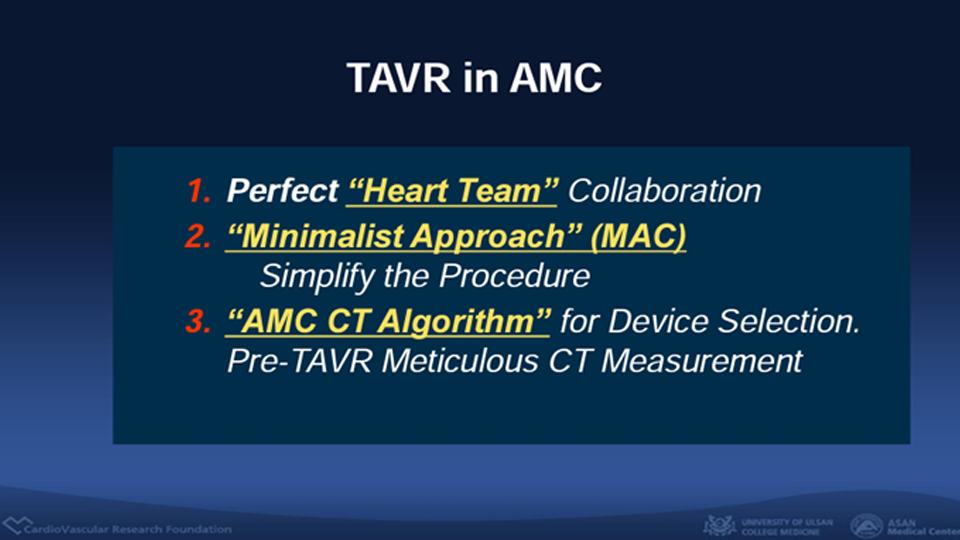
This success can be attributed to a collaborative heart team approach, a minimalist approach known as MAC (Monitored Anesthesia Care), and a meticulous AMC CT algorithm for device selection. The AMC CT Algorithm is a major key to achieving a procedural success rate of 99.5%. This algorithm can identify various anatomical factors, including annulus area, calcium distribution, and coronary height, which are measured to determine the size of the valve and its suitability for TAVR. The choice of TAVR device and balloon volume is determined by the level of calcium and other structural factors. The data from AMC’s TAVR procedure show favorable 30-day and 1-year outcomes, including all deaths (1.5%, 8.4%, respectively), cardiac death (1.1%, 2.2%, respectively), and disabling stroke (1.3%, 1.4%, respectively).
In conclusion, Dr. Park emphasizes that TAVR has become the standard of care for patients with symptomatic severe aortic stenosis, regardless of age or specific cases. SAVR is considered primarily for patients who are unsuitable for TAVR. The data and experience of AMC presented to support the effectiveness of the heart team approach, the minimalist MAC procedure, and the CT algorithm for valve size selection, highlighting their key factors for success.
Edited by

Jinho Lee, MD
Kyung Hee University Medical Center, Korea (Republic of)

KyungAe Kim, RN
CardioVascular Research Foundation (CVRF), Korea (Republic of)
Seung-Jung Park, MD, PhD (Asan Medical Center) presents the 14-year journey of TAVR in the opening session during the 12th AP VALVES & STRUCTURAL HEART 2023 held at the Grand Walkerhill Seoul, South Korea on August 10.
As of 2023, the 2020 ACC/AHA guideline recommends TAVR for severe symptomatic Aortic Stenosis (AS) patients over the age of 65, while those under 65 are considered for Surgical Aortic Valve Replacement (SAVR) based on their age. However, the 2021 ESC/EACTS guidelines recommend TAVR for patients over 75 years of age, with all other patients evaluated for either TAVR or SAVR based on their specific condition. Dr. Park now suggested that TAVR is the primary choice for patients in need of a tissue valve, with SAVR considered for those deemed unsuitable for the TAVR procedure.
Asan Medical Center, which initiated TAVR procedures in 2010 and currently performs approximately 300 TAVR cases per year, totaling over 1500 cases, has achieved promising outcomes. These outcomes include procedural success rates of 99.5%, with low mortality (1.3%), stroke (0.3%), vascular complications (4.2%), permanent pacemaker insertion (6.8%), moderate to severe paravalvular regurgitation (0.4%), and more, showcasing the effectiveness of their approach.
This success can be attributed to a collaborative heart team approach, a minimalist approach known as MAC (Monitored Anesthesia Care), and a meticulous AMC CT algorithm for device selection. The AMC CT Algorithm is a major key to achieving a procedural success rate of 99.5%. This algorithm can identify various anatomical factors, including annulus area, calcium distribution, and coronary height, which are measured to determine the size of the valve and its suitability for TAVR. The choice of TAVR device and balloon volume is determined by the level of calcium and other structural factors. The data from AMC’s TAVR procedure show favorable 30-day and 1-year outcomes, including all deaths (1.5%, 8.4%, respectively), cardiac death (1.1%, 2.2%, respectively), and disabling stroke (1.3%, 1.4%, respectively).
In conclusion, Dr. Park emphasizes that TAVR has become the standard of care for patients with symptomatic severe aortic stenosis, regardless of age or specific cases. SAVR is considered primarily for patients who are unsuitable for TAVR. The data and experience of AMC presented to support the effectiveness of the heart team approach, the minimalist MAC procedure, and the CT algorithm for valve size selection, highlighting their key factors for success.
Edited by
Jinho Lee, MD
Kyung Hee University Medical Center, Korea (Republic of)
KyungAe Kim, RN
CardioVascular Research Foundation (CVRF), Korea (Republic of)
Leave a comment