
News | TCTAP 2024
DCB Use in Your PCI Practice: Adjunctive Therapy or Standard of Care?
Evolving PCI Devices: Coronary DES, BRS, and DCB

Bruno Scheller
University of Saarland, Germany
Despite advancements in interventional procedures, that began with the development of balloon angioplasty by Andreas Grüntzig in 1977, stent-related adverse events occur in approximately 2-3% of cases every year. DCB was developed based on its unique, "leave nothing behind" philosophy. Since co-developing the first DCB with Ulrich Speck in the late 1990s, Sheller’s innovations have significantly advanced the field of interventional cardiology. DCBs are expected to reduce the number and length of stents without causing stent-related adverse events, and much research is currently being conducted.
Efficacy of DCBs compared to DES
At the conference, recent studies will be presented, which demonstrate that DCBs are equivalent to drug-eluting stents (DES) for stent restenosis when appropriate lesion preparation is performed. Based on this research, DCBs were recommended as an option for the treatment of in-stent restenosis (ISR) in the 2018 European Society of Cardiology (ESC) Guideline.
On the contrary, the use of DCB for de novo lesions of small coronary artery lesions has not yet been included in the guidelines, due to the lack of data. The benefits of DCB application in de novo vessels will be introduced through studies such as the BASKET-SMALL 2 trial and DEBUT trial. In the BASKET-SMALL 2 trial, which investigated non-inferiority for treatment with DCB compared with DES in patients undergoing PCI for de novo lesions in small coronary arteries, 8 patients presented with a complete thrombotic vessel occlusion after undergoing stent implantation compared to none after a DCB intervention. Meanwhile, there was no difference in the estimates of the cumulative probabilities of major adverse cardiac events (MACE) in the two study groups over 3 years.
Optimal lesion preparation has been mentioned as the most important factor in applying DCB strategy. It is necessary to assess whether lesion preparation for DCB is adequate. DCB may be a good alternative to DES for cases where the residual stenosis is ≤ 30% and fractional flow reserve (FFR) is > 0.8, with absence of flow limiting dissection during the lesion preparation process (Figure 1). The choice of DCB and DES should be determined based on whether optimal angiographic findings are obtained after lesion preparation.
Additional strengths of DCB
Post-procedural late lumen enlargement (LLE) and vasomotion will be presented as additional strengths of DCB. According to a study assessing intravascular geometric and compositional characteristic changes induced by DCB in de novo lesions, LLE after DCB treatment for de novo coronary artery disease (CAD) was caused by both vessel enlargement and plaque regression. Similarly, according to a study which compared coronary vasomotion in patients with small CAD treated with DCB versus DES, vasoconstriction after acetylcholine infusion in the peri-treated region was less pronounced in the DCB arm than in the DES arm. This suggests that endothelial function in treated coronary vessels could be better preserved by DCB than by new-generation DES. In case of patients with multivessel CAD, the application of DCB provided benefits compared to utilizing DES only with regard to the risk of MACE over 2 years.
Due to these strengths and developments in DCB, the adoption rate of DCB is gradually increasing worldwide. According to the coronary DCB to DES ratio in PCI worldwide, in 2020 this ratio was 1:25 in Europe, which has increased to 1:4 in 2023. This trend reflects growing confidence in the efficacy and safety of DCBs due to successful clinical outcomes and growing support from the medical community.
The presentation will highlight the historical advancements and current achievements of DCB technology, as well as its potential to revolutionize cardiac care. Based on the studies presented, it can be expected that DCB will develop into a standard of care rather than simply adjunctive therapy. As the field seeks less invasive and more effective treatments, ongoing research, including Scheller's, and advocacy for DCB will likely play a pivotal role in setting new standards in cardiovascular medicine.
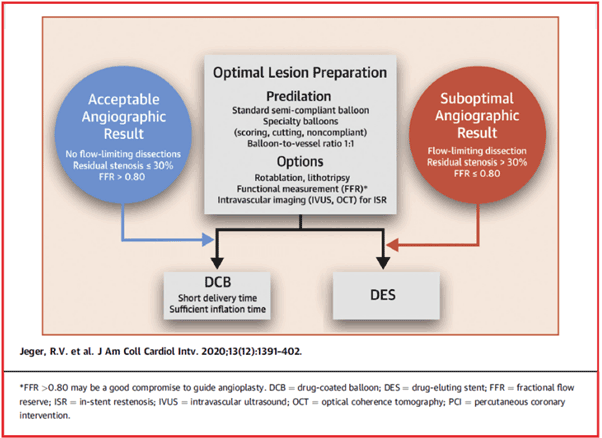
Figure 1. DCB-only strategy for PCI in CAD
TCTAP Workshops
Evolving PCI Devices: Coronary DES, BRS, and DCB
Thursday, April 25, 4:50 PM ~ 5:50 PM
Presentation Room 1, Level 1
Edited by

Sang Yong Jo, MD
Dong-A University Hosital, Korea (Republic of)
Bruno Scheller
University of Saarland, Germany
Despite advancements in interventional procedures, that began with the development of balloon angioplasty by Andreas Grüntzig in 1977, stent-related adverse events occur in approximately 2-3% of cases every year. DCB was developed based on its unique, "leave nothing behind" philosophy. Since co-developing the first DCB with Ulrich Speck in the late 1990s, Sheller’s innovations have significantly advanced the field of interventional cardiology. DCBs are expected to reduce the number and length of stents without causing stent-related adverse events, and much research is currently being conducted.
Efficacy of DCBs compared to DES
At the conference, recent studies will be presented, which demonstrate that DCBs are equivalent to drug-eluting stents (DES) for stent restenosis when appropriate lesion preparation is performed. Based on this research, DCBs were recommended as an option for the treatment of in-stent restenosis (ISR) in the 2018 European Society of Cardiology (ESC) Guideline.
On the contrary, the use of DCB for de novo lesions of small coronary artery lesions has not yet been included in the guidelines, due to the lack of data. The benefits of DCB application in de novo vessels will be introduced through studies such as the BASKET-SMALL 2 trial and DEBUT trial. In the BASKET-SMALL 2 trial, which investigated non-inferiority for treatment with DCB compared with DES in patients undergoing PCI for de novo lesions in small coronary arteries, 8 patients presented with a complete thrombotic vessel occlusion after undergoing stent implantation compared to none after a DCB intervention. Meanwhile, there was no difference in the estimates of the cumulative probabilities of major adverse cardiac events (MACE) in the two study groups over 3 years.
Optimal lesion preparation has been mentioned as the most important factor in applying DCB strategy. It is necessary to assess whether lesion preparation for DCB is adequate. DCB may be a good alternative to DES for cases where the residual stenosis is ≤ 30% and fractional flow reserve (FFR) is > 0.8, with absence of flow limiting dissection during the lesion preparation process (Figure 1). The choice of DCB and DES should be determined based on whether optimal angiographic findings are obtained after lesion preparation.
Additional strengths of DCB
Post-procedural late lumen enlargement (LLE) and vasomotion will be presented as additional strengths of DCB. According to a study assessing intravascular geometric and compositional characteristic changes induced by DCB in de novo lesions, LLE after DCB treatment for de novo coronary artery disease (CAD) was caused by both vessel enlargement and plaque regression. Similarly, according to a study which compared coronary vasomotion in patients with small CAD treated with DCB versus DES, vasoconstriction after acetylcholine infusion in the peri-treated region was less pronounced in the DCB arm than in the DES arm. This suggests that endothelial function in treated coronary vessels could be better preserved by DCB than by new-generation DES. In case of patients with multivessel CAD, the application of DCB provided benefits compared to utilizing DES only with regard to the risk of MACE over 2 years.
Due to these strengths and developments in DCB, the adoption rate of DCB is gradually increasing worldwide. According to the coronary DCB to DES ratio in PCI worldwide, in 2020 this ratio was 1:25 in Europe, which has increased to 1:4 in 2023. This trend reflects growing confidence in the efficacy and safety of DCBs due to successful clinical outcomes and growing support from the medical community.
The presentation will highlight the historical advancements and current achievements of DCB technology, as well as its potential to revolutionize cardiac care. Based on the studies presented, it can be expected that DCB will develop into a standard of care rather than simply adjunctive therapy. As the field seeks less invasive and more effective treatments, ongoing research, including Scheller's, and advocacy for DCB will likely play a pivotal role in setting new standards in cardiovascular medicine.
TCTAP Workshops
Evolving PCI Devices: Coronary DES, BRS, and DCB
Thursday, April 25, 4:50 PM ~ 5:50 PM
Presentation Room 1, Level 1
Edited by
Sang Yong Jo, MD
Dong-A University Hosital, Korea (Republic of)
Leave a comment